Standers with Hip Abduction
The majority of therapeutic standers being introduced into the market today have options for hip abduction (legs moved out to the side away from midline) while standing. Why?

The answer has to do with development of a healthy hip joint.
Hip Anatomy and Terminology
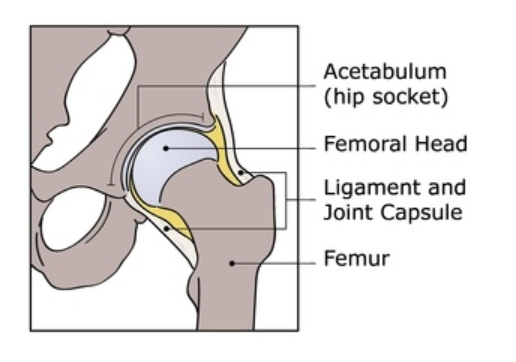
"The hip is the largest “ball-and-socket” joint in the body. It is held together by ligaments, tendons, and a joint capsule.
The ball is called the “femoral [fem-er-uhl] head,” which is the top of the femur or thigh bone.
The socket is called the “acetabulum” [as-i-tab-yuh-luhm] and is a part of the pelvis.
The femoral head fits into the acetabulum forming the hip joint. They fit together so the ball can rotate freely in the socket."
- International Hip Dysplaysia Institute https://hipdysplasia.org/adults/
Understanding Hip Dysplasia
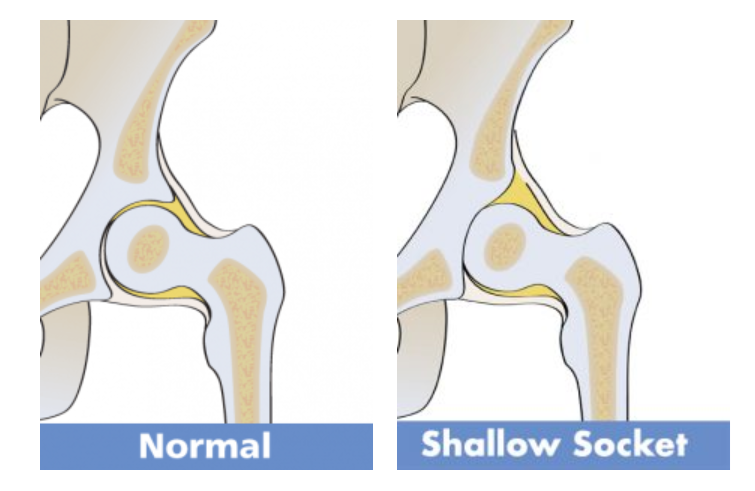
Weightbearing through the legs in standing is the force that presses the head of the femur into the acetabulum or the “ball” into the “socket”. Without these weight bearing forces, for example in child who does not begin to stand and walk at an age-appropriate time (usually between the ages of 9 to 18 months), the acetabular “cup” does not deepen as it should. A shallow socket, especially in the presence of weak and spastic hip muscles, which is common in children with developmental disabilities such as cerebral palsy, can lead to hip migration.
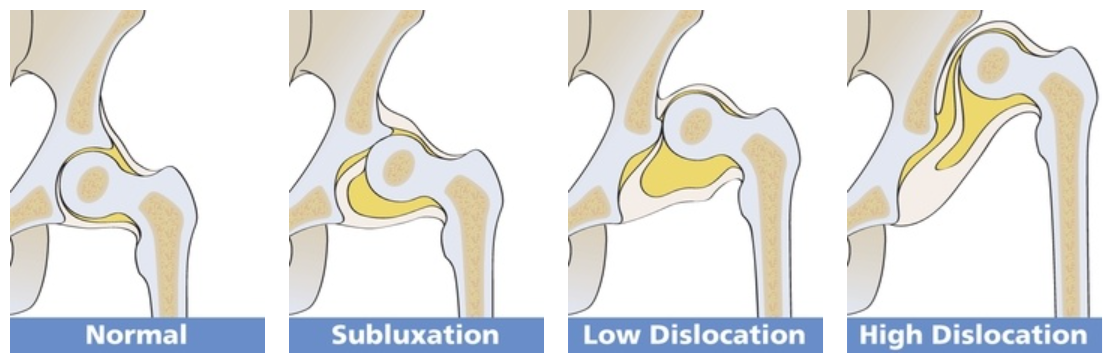
Hip migration is movement of the head of the femur out of the acetabulum. Subluxation is the term used when the head of femur is partially moved outside of the acetabulum. Dislocation is considered full movement of the head of the femur outside of the acetabulum.
Hip migration is very common in children with cerebral palsy. It is caused by a combination of factors including:
- Spastic Muscles that pull atypically on the anatomy of the hip. Spastic muscles (muscles with increased muscle tone) also tend to be “tight” meaning over time they can lose their elasticity. Eventually they may permanently shorten which can cause loss of range of motion (movement) at the hip. It is usually spasticity in the muscles that positions the hip in flexion (bending up towards trunk), adduction (moving thigh towards midline and sometimes crossing over the other leg) and internal rotation (rotating knee inward) that can displace the femoral head.
- Weak Muscles are frequently seen in combination with spastic muscles as the typical balance between muscle groups is disturbed. Usually the abductor muscles, the muscles that move the leg out to the side are weak. This can contribute to the head of the femur being somewhat misshapen because it does not seat itself properly in the acetabulum.
- Delayed Weight Bearing as described earlier in this article.
Monitoring the hips for migration out of typical alignment using frequent x-rays and physical exam is important because this process is often asymptomatic (lacks physical cues that something is happening). And, hip migration is often progressive. If identified early, hip migration can be slowed or reversed. This can improve hip health when bones reach maturity. Without treatment the acetabulum does not form correctly, the head of the femur can become mishappen and subluxation or dislocation can result. This can cause pain, limit range of motion, and make it difficult to sit let alone stand and walk.

Standing in standers that are able to support the legs in abduction (legs moved away from midline forming an inverted “V”) have been researched over the past several decades showing promising results of improved hip health in at risk populations. Standing with hips abducted 10 to 30 degrees for each hip for an hour daily puts a prolonged stretch on the muscles on the inside of the thigh helping to preserve range of motion. Weightbearing with a prolonged stretch can also help to manage increased muscle tone in these muscles. The position of legs abducted also firmly positions the head of the femur in the acetabulum while weightbearing which helps to deepen the acetabulum. A standing program with legs abducted has also been found beneficial to individuals who have needed surgery to lengthen shortened muscles around the hip that have begun to cause hip migration.
For further information on research studies and supporting documents please explore resources below.
Resources:
- Effects of the standing program with hip abduction on hip acetabular development in children with spastic diplegia cerebral palsy.
- Abducted Standing in Children with Cerebral Palsy: Effects on Hip Development After 7 Years
- Standing Programs to Promote Hip Flexibility in Children with Spastic Diplegic Cerebral Palsy
- Effects of the standing program with hip abduction on hip acetabular development in children with spastic diplegia cerebral palsy
- Inclination, hip abduction, orientation, and tone affect weight-bearing in standing in standing devices.
- Hip Surveillance and Management of Hip Displacement in Children with Cerebral Palsy: Clinical and Ethical Dilemmas
- Etiology of Hip Displacement in Children with Cerebral Palsy
- Evidence Update: Long-Term Benefits of Abducted Standing in Children with Cerebral Palsy
- Supported Standing, what does the research say?
